
10. The Timeline

‘Morning, Jane!’
I didn’t have any new admissions that Thursday, so I had seen all of my inpatients by 10am. That means I actually had time to take my mid-morning coffee in the cafeteria, an accomplishment that took me four months of residency to get it.
At the table I could hear Jax laughing behind me, I turned around and saw him at a table with the other pediatrics residents. When he saw me, he came and sat across from me.
‘Hey, Liz! What a surprise.’
‘I know! It’s the first day ever that I finished everything before the rounds.’
‘Good for you!’
‘Don’t you people have work in peds? How come all the residents are free at this time of the day?’
‘Well, Holmes took a couple of weeks off, and it turns out our new attending loves that we fraternize and eat well before the rounds.’ He smiled broadly. ‘She’s actually there with us.’ He pointed at a glowing woman, ‘Dr. Torelli, you would love her.’
‘Nice! Good for you then.’
A couple of seconds later, Peter sat beside me and stretched his arm to greet Jax.
‘Hi, I’m Peter.’ He smiled.
‘Oh, so this is Peter! Nice to meet you, Peter. I’m Jax, Lisa’s roommate.’
‘Wait, do you all come here in the mornings?’ I turned to Peter. ‘Am I the only one who gets stuck in paper work?’
They both laughed.
At 11am me and Peter were already with Dr. Collins at her office. We went through the follow ups on my patients first, and then to Peter’s admission.
‘So, today one of my outpatients was admitted.’ He started with a worried expression. ‘William Grant, 52 years old. He comes to the clinic regularly because of a 3-year history of migratory arthralgias affecting mostly the knees, elbows and wrists. He had been using methotrexate and steroids which moderately controlled his pain. He was admitted today with diarrhea. His last appointment at the clinic was with me, a month ago.’
‘I see.’ Lucy said before he continued. ‘I think he deserves a timeline Peter, don’t you think?’
For more complex cases with longer medical history, Dr. Collins encouraged us to present the case as a timeline. That way, the associations of each of the patient’s problems became more clear. It was actually super fun, I loved timeline days.
‘I do!’ he said while I got up to get the white board from behind the door.
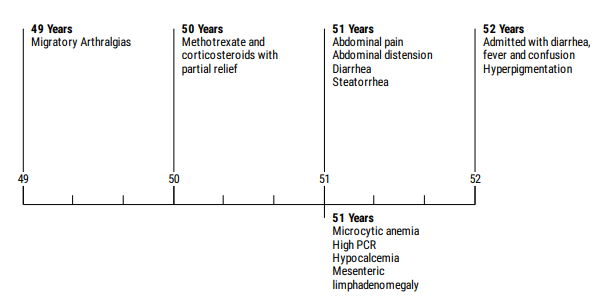
‘So, William Grant, 52 years old, farmer. Previously healthy with no medical history until three years ago.’ he said as I was writing on the board. ‘When he started with a migratory arthralgia involving knees, elbows and wrists.’ he paused.
‘A year later he started a treatment with methotrexate and corticosteroids that partially improved his symptoms. His workup back then didn’t point to any specific diagnosis.’
‘Ok.’ I said finishing the writing. ‘Go on.’
‘Then 6 months ago he started with intermittent abdominal pain and distension precipitated by food. So he came to his appointment with me 1 month ago with those complaints. He also told me he had some episodes of diarrhea with steatorrhea during this time and had lost some weight, but didn't know how much.’
‘That’s good, Peter. What did you do then?’ Lucy asked.
‘Well, I ordered some blood work for him at the time, a fecal occult blood test and also an abdominal ultrasound. Of those, the blood work showed a microcytic and hypochromic anemia, increased PCR and hypocalcemia. And the ultrasound showed mesenteric lymphadenomegaly.’
‘Interesting. And what brought him here today?’
‘Today he was brought by his family because his abdominal pain and diarrhea got worse. Beyond that, his wife said he has been confused for the past days and has had some memory losses.’
‘Okay. Anything on the physical exam?’ Lucy seemed intrigued.
‘He had a slight fever. Nothing else of note.’
‘What about anything else at all?’
‘Well, his skin seemed a little hyperpigmented I think.’
‘Right. So, a man with arthralgias for years, now with diarrhea, abdominal pain, weight loss and apparently confusion. What do you guys think?’
We started to think about possible diagnosis that could explain his symptoms. All sorts of possibilities came up on the board. Inflammatory bowel disease, seronegative polyarthritis, Celiac, gastroenteritis, cancer and even TB, cause who knows, it may always be TB.
‘Those are all important conditions for our differential.’ Lucy responded. ‘But there’s one that you haven’t mentioned yet, which I think deserves a spot there.’
We waited in silence.
‘It could be a specific infection. More commonly seen in caucasian men and that causes malabsorption syndrome.’
Peter and I looked at each other. Nothing yet. What were we missing?
‘Well, I’ll let you think about it for a moment. I need to sign some papers at the reception and will be right back.’
She left and I turned to Peter ‘Damn, what is it?’
‘No clue. Maybe it’s not related after all... The arthralgias and diarrhea.’
‘Maybe. But I don’t think so, Lucy hinted that this infection could explain everything.’
‘Yeah, she did.’ Peter buried his head in his hands. ‘William seems so confused, his wife is worried sick. I should have asked myself more questions a month ago.’
I reached for his shoulder ‘It happens, Peter. You ordered his workup and did what any of us would have done. We are going to get it this time.’
Dr. Collins walked in again.
‘One more hint then.’ she continued. ‘First name of the bacteria is Tropheryma.’
‘Whipple’s.’ we automatically said together. Unbelievably obvious, wasn’t it?
Lucy smiled. ‘Yes. The arthralgias, confusion, diarrhea and mesenteric lymphadenopathy makes it a good option. And Mr. Grant also has hyperpigmented skin to seal the deal. So anyway I think a biopsy could help us, right?’
Peter ordered a small bowel biopsy for Mr. Grant that day. As Lucy predicted we later received the results: beautiful PAS-positive foamy macrophages invading the lamina propria. William was treated with IV ceftriaxone in the hospital and after some time was discharged with oral TMP-SMX for maintenance.
‘Hey, William is going to be okay.’ I said as we were leaving the hospital that day.
Peter smiled. ‘Yeah, he is.’
…
Want to know more about Whipple’s disease?
https://rarediseases.info.nih.gov/diseases/7889/whipple-disease
Want to read real cases of Whipple’s disease?
https://www.scielo.br/scielo.php?pid=S0036-46652001000100009&script=sci_arttext
Clinical Board

RF: risk factors; SS: signs and symptoms; CNS: central nervous system;
TMP-SMX: trimethoprim/sulfamethoxazole.










No comments: